Fostering social participation — defined as involvement in activities that provide interactions with others in the community — is crucial not only for allowing older adults to meet their fundamental human needs for socialization and self-actualization, but for helping society to better face population aging. Currently, approximately half of older adults have restricted social participation. Because such participation is a critical element of older adults’ health, its decline has been associated with serious health outcomes, including a 29 percent greater risk of mortality.
The challenge of helping elderly people to maintain social participation is targeted in a limited way in the 2018-23 Action Plan Un Québec pour tous les âges. While this plan mainly focused on economic activities like labour force participation, an important aspect of maintaining or increasing social participation is optimizing a person’s abilities and environment by, for example, improving mobility or providing an environment that promotes interactions.
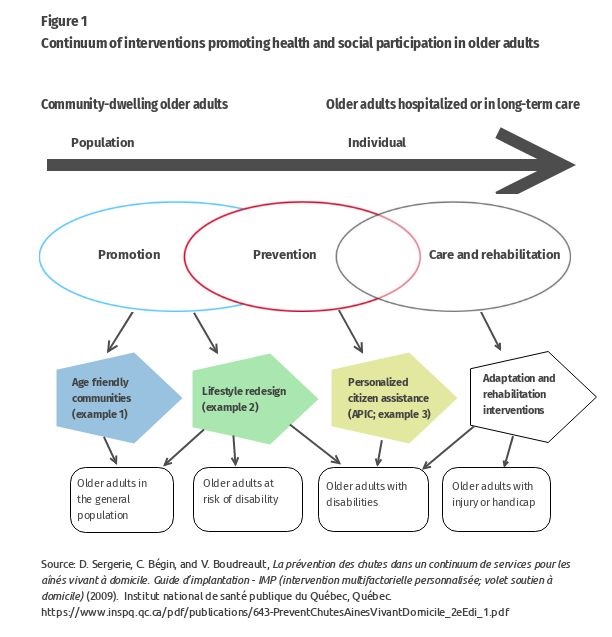
One approach that a team at the Research Centre on Aging has developed to promote social participation is the concept of a continuum of interventions (figure 1) at the levels of the individual and the population. The continuum includes adapting communities’ services and structures to help aging adults live safely, enjoy good health and stay involved in their communities (example 1); and personalized interventions (examples 2 and 3) fostering empowerment, utilization of personal resources and accomplishment of social activities for as many older adults as possible.
Research indicates that interventions to strengthen social participation should:
- last at least six months
- recruit older adults in their own living environments and build community partnerships
- be personalized by acknowledging and respecting the interests, needs, experiences and culture of older adults
- support the development of meaningful social relationships and roles
- foster real partnerships with older adults
Although some social participation opportunities exist in Canada, community organizations, health professionals and municipalities don’t pay enough attention to older adults’ personal and environmental resources, are not sufficiently personalized or do not suitably build partnerships. As well, they mainly reach more educated people so they in fact increase inequalities in health outcomes.
In addition to the existing adaptation and rehabilitation services (outlined in figure 1), three particular interventions that have the potential to improve current practices are age-friendly communities (AFCs), the Lifestyle Redesign program and Accompagnement citoyen personnalisé d’intégration communautaire (personalized citizen assistance for social participation, or APIC).
Age-friendly communities (AFCs) (example 1 in figure 1) encourage active aging by adapting structures and services so they are to be accessible for and inclusive of older people with varying needs and capacities. For example, ensuring there are sidewalks, controlling traffic density and speed, minimizing the distance to and increasing the accessibility of buildings that provide physical and social activities improve older adults’ mobility and social participation. However, while AFC are believed to be one of the best ways to help older adults lead healthy and active lives and stay involved in their communities, it is essential that researchers identify how these age-friendly communities get results and which specific aspects of them are most conducive to improving health outcomes and equality, and to social participation. As well, identifying which communities are more suitable for implementation of interventions such as Lifestyle Redesign or APIC is also important.
Lifestyle Redesign is a preventive occupational therapy intervention empowering older adults to increase their social participation by regularly performing activities to achieve healthy and fulfilling lives (example 2 in figure 1). Offered over six to nine months, Lifestyle Redesign includes weekly two-hour group sessions and individual monthly meetings. During these sessions, an occupational therapist covers various topics through presentations, peer exchanges, reflective exercises, direct experience and personal exploration. Studies in the United States have shown that Lifestyle Redesign fosters significant positive changes in the participants’ bodily pain, vitality, social and mental functioning, and overall life satisfaction. About 90 percent of the participants experienced improvements lasting for at least six months after the end of the intervention, and these improvements were cost-effective. The health care costs of participants in the Lifestyle Redesign group were less than a third of those of people who did not participate in the group. In a Canadian study, the Research Centre on Aging demonstrated that, when adapted to Canada, Lifestyle Redesign helped older people to pursue meaningful activities and healthy lifestyles. Further study of the cost effectiveness and impact of this intervention is needed.
APIC (example 3 in figure 1) consists of weekly three-hour personalized stimulation sessions over 6 to 12 months, where nonprofessional attendants work individually with older adults with disabilities to help them accomplish significant social and leisure activities in the community such as joining a group to do physical activities. During these sessions, attendants help older adults to have a better knowledge of community resources, target goals for significant social and leisure activities that were difficult to accomplish and encouraged empowerment, gradual mobilization of personal and environmental resources, and community integration. Attendants had two days of training and were supervised by the research team. It has been shown that APIC can increase older adults’ mobility, accomplishment of social activities and frequency of leisure activities. By complementing and extending professional health care services, APIC helped older adults with disabilities to resume, maintain, explore and experiment with significant social activities. It increased their psychological and physical well-being, feeling of control, connectedness, self-esteem and motivation to accomplish activities. These results indicate the need to further evaluate APIC, especially when it is conducted by volunteers supervised by coordinators in community organizations.
These three interventions can improve the services offered by community organizations, health professionals and municipalities. They would also help older individuals to better meet their social participation needs, use their abilities, enjoy the respect and esteem of others, and maintain meaningful relationships. Over the long term, older adults would be healthier and have less need for health and social services. Society could benefit from the experience and contribution of older adults (for example, if they did volunteer work). These interventions might result in other benefits; for example, improving the accessibility of health services and reducing their costs.
Canada’s population is aging and chronic disease rates are increasing, but hospital stays are shorter, long-term care is less available, and health care budgets are being reduced. There will be elder adults needing supportive environments such as age-friendly communities, they will need preventive interventions like those offered by Lifestyle Redesign, and they will need to be assisted by volunteers (APIC). Mostly carried out in the community, for women and men, across cultural and economic conditions, interventions such as these may help in situations where health professionals have limited knowledge of their patients and not enough time to spend with each patient, which results in fewer interventions and less follow-up.
Photo: Shutterstock, by Robert Kneschke
Do you have something to say about the article you just read? Be part of the Policy Options discussion, and send in your own submission. Here is a link on how to do it. | Souhaitez-vous réagir à cet article ? Joignez-vous aux débats d’Options politiques et soumettez-nous votre texte en suivant ces directives.