Our health is global. Our country’s ability to prepare for, prevent and respond to the spread of infectious diseases is deeply connected to the ability of other countries to do the same. Yet to date, Canada’s response to COVID-19 has been assessed mostly in terms of actions taken within its own borders.
Concerns have been raised on a number of fronts: the inability to ramp up testing and tracing, the failure to stockpile personal protective equipment (PPE) and ventilators, failure on the part of the provinces to share public health data with the federal government (a need previously underscored during the severe acute respiratory syndrome, or SARS, crisis), and the appalling conditions, magnified by COVID-19, of too many long-term care homes. On the rare occasion that Canada has looked up and outward, it has largely been to congratulate itself for avoiding the freefall happening in the United States.
But COVID-19 is a global pandemic, and so we also need to examine Canada’s neglect of its global role and how that has contributed to the spread of COVID-19 both in Canada and elsewhere.
In our new book, Vulnerable: The Law, Policy and Ethics of COVID-19, contributors highlight truths that global health scholars have espoused for decades. In 2020, harmful infectious threats no longer take years to spread across borders; they need mere hours via long-haul international flights.
And if primarily wealthy countries make the international rules about what is required to prepare and respond to disease outbreaks, it is unlikely countries with vastly fewer resources will be protected. Global health threats such as climate change, antimicrobial resistance and new and re-emerging infectious diseases have shown us that our health is interconnected, and some of us – individuals, groups, and countries – are more vulnerable than others as a result. Unless we attend to these vulnerabilities, none of us can adequately protect ourselves.
Poverty has proven to be a key factor in the spread of COVID-19. Poverty makes people vulnerable and constrains their ability to protect themselves from imminent threats. Overcrowded, substandard housing combined with pre-existing health conditions that already limit life expectancies and under-resourced healthcare systems create conditions for contagion to spread quickly and deeply into populations. Social distancing – the mainstay of prevention efforts – is a luxury of the middle and upper classes.
The World Health Organization (WHO) began providing clear messaging in January that countries should test, isolate, trace and treat. And despite the fact the WHO did not recommend border closures, countries worldwide began shutting down their borders.
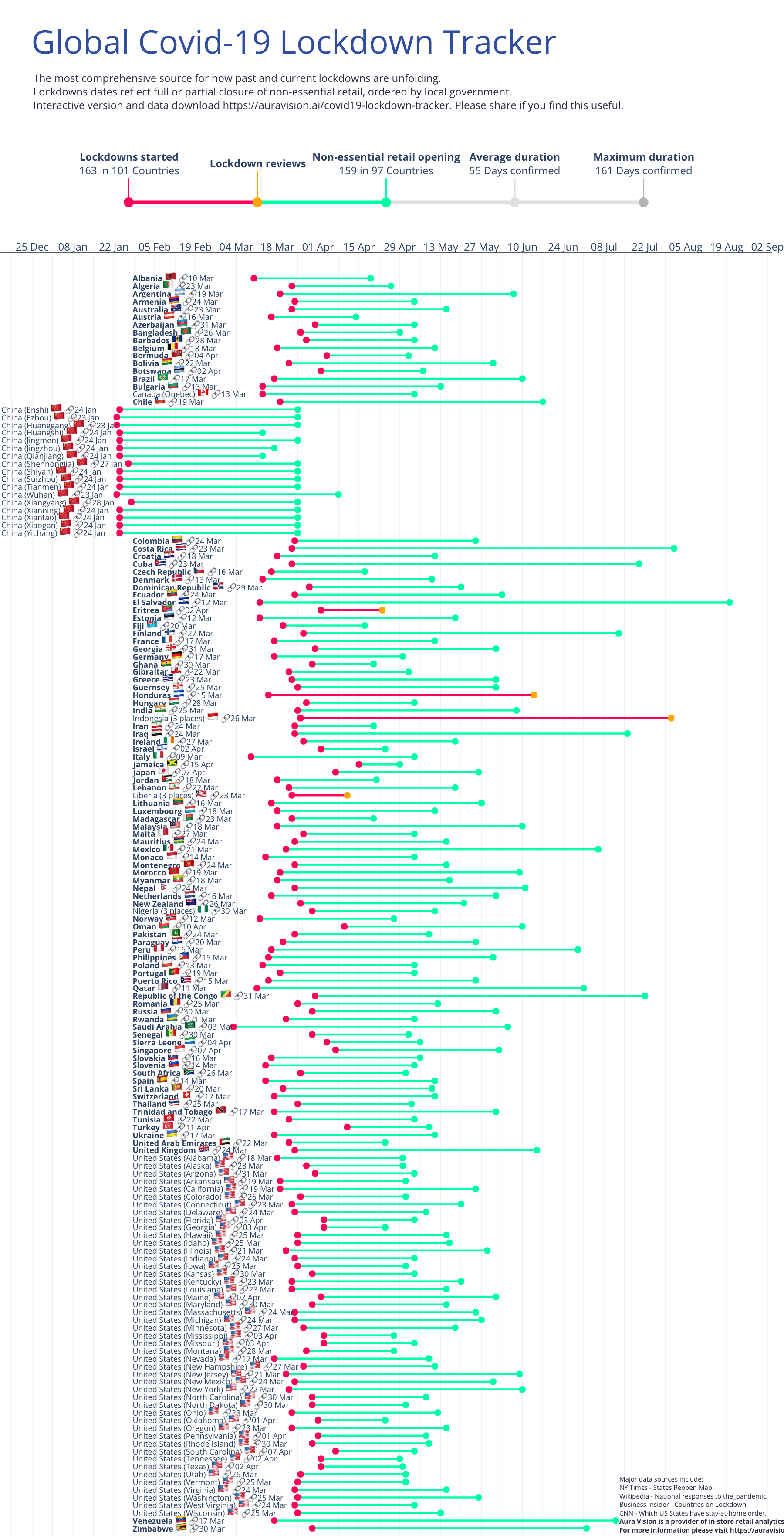
Following China’s and Italy’s examples, most countries began self-quarantining or implementing lockdowns by mid-March. How and why national lockdowns become the primary policy of government leaders is still unclear. Lockdowns were not the only or most effective option. In low and middle-income countries (LMICs), lockdowns produced staggering hardships for hundreds of millions of people.
The implausibility of following physical distancing for many in LMICs, combined with governments’ inability to provide a safety net for citizens during lockdown, meant the science-based “one-size-fits-all” pandemic responses had devastating consequences.

In India, millions of rural to urban migrants who survive on daily wages were suddenly left with no work or cash to pay for housing. Millions took to the roads, walking for hundreds of kilometres back to their ancestral villages and towns. In many LMICs, where millions live in densely populated slums, the basic prerequisites for lockdown survival such as clean water, toilets, space, savings to buy food, refrigerators and internet do not exist. Some venturing out in desperation for work or food were brutally beaten by police for breaking lockdown restrictions.
As nations around the world fumble through their response to COVID-19 with more or less success, the early experience reveals the desperate need for a well-resourced, central agency to spread the best scientific evidence on precautions and treatments for differently situated countries, and distribute resources to those countries that need additional support to control COVID-19. The WHO has become a punching bag for many countries even though it has deemed its annual budget of just $4.8 billion adequate for all health programs for the entire globe. Countries have not been willing to increase their dues, leaving the WHO highly politicized because of its dependence on the largess of nation states and foundations.
The “us-versus-them” politics has begun to surge again in the context of vaccines as it first did with the global competition for PPE and ventilators. Which country will discover the vaccine first, who will get it first and will LMICs get the vaccine? These are all open questions. On May 4, the G20 countries, except the US and Russia, joined major philanthropists to raise nearly 8 billion euros (approximately $12.3 billion Canadian) for research and development of diagnostics, therapies and vaccines. They promised these would all be public goods, and fairly distributed. Meanwhile, private sector companies, most based in the US, are also racing to develop vaccines, which will be distributed via the market.

Let us be clear: a world in which a vaccine and other treatments are not made available for all will exacerbate existing health inequalities and poverty. And sooner or later these conditions will help spread the current or other novel diseases, and the next global pandemic.
Global ethics once centred around the axis of our national wellbeing versus those of foreigners. That paradigm is no longer viable, either as a matter of domestic public health or global ethics. In our interconnected and interdependent world, protecting ourselves requires raising the quality of life and health resilience of everyone.
Canada’s foreign aid flows now represent 0.27 percent of Gross National Income, an amount lower than when Stephen Harper was prime minister. While the government has announced some foreign aid to combat the coronavirus, it is far too low to provide the real help on the ground that so many countries need. Our financial, scientific and political contributions are far too modest for Canada to step up into a global leadership role in response to COVID-19, much less fill the void left by the US’s withdrawal from the WHO, which resulted in the loss of its largest source of funding.
But even a country of Canada’s modest size can provide global leadership. For example, it could lead in reforming international health regulations, which need to be reviewed in light of COVID-19. It could also make a significant new fiscal contribution to the WHO – with no strings attached – and calibrate those contributions so that if similar percentage increases were made by other countries it would fill the void left by the US. This global crisis is an opportunity for Canada to lead the world in global public health, and it should seize it for the long-term interests of Canadians and all human beings.
The authors are co-editors, with Jane Philpott and Sophie Thériault, of Vulnerable: The Law, Policy and Ethics of COVID-19, out now and available open access from University of Ottawa Press.
This article is part of the Addressing Vulnerabilities for a More Equitable Pandemic Response special feature.












{kind=link}