



“Behold: a new $829 billion entitlement that will subsidize insurance for tens of millions of people — and reduce deficits by $81 billion at the same time. In the next tent, see the mermaid and a two-headed cow.”
The Wall Street Journal
If you want further illustration of the intensity of the debate around health care reform and the language of “public option” and ‘individual mandate’, google the snippets from the toxic town halls last summer and listen to the heated exchanges on “death panels” by the pistol-packing participants.
Americans, the late Senator Daniel Patrick Moynihan told me many years ago, take their politics seriously, and to suggest otherwise is not to have read American history. At its extreme the health care debate pits rich against poor, seniors against youth, and exacerbates political polarization. It can also be funny and informative — watch, for example, Will Ferrell’s viral video with Mad Men‘s Jon Hamm and other Hollywood celebs. It is politicking in the raw.
The first Democratic candidate to win a majority of the vote since 1976, the public embrace of Barack Obama and his promise of “Change We Can Believe In” has a fillip not seen since Jimmy Carter’s election under the slogan “A Leader, For a Change” (although Carter’s presidency is a cautionary tale of unfulfilled promise). In its scope and scale the reformist agenda of President Obama — the stimulus package, health care, climate change, launched during his first year with the promise to tackle education and immigration reform in 2010 — rivals the ambitions of Franklin Roosevelt’s New Deal and Lyndon Johnson’s Great Society. He does this against the backdrop of a recession and, for now, a jobless recovery. Added to this are two wars — an endgame in Iraq and a “war of necessity’ in Afghanistan — along with the Middle East, all of which may yet determine the credibility of his recently awarded Nobel Peace Prize.
Obama has made health care his signature issue. As he told the American Medical Association in June: “Make no mistake: the cost of our health care is a threat to our economy. It’s an escalating burden on our families and businesses. It’s a ticking time-bomb for the federal budget. And it is unsustainable for the United States of America.”
Obama aims to succeed where every president, going back to Teddy Roosevelt, has either faltered or failed. The outcome will be important when history delivers its verdict on America’s 44th president. The breadth and comprehensiveness of health care reform have dominated the congressional agenda for the past six months, effectively squeezing out other agenda items, including climate change.
Politically it is extraordinarily ambitious. It means taking on a sector that represents one-sixth of American GDP and interests that include the medical profession, the drug industry, insurers and seniors. Reform would change the lives of all Americans, especially the more than 133 million Americans living with chronic diseases and disabilities and their family caregivers.
For the “lion of the Senate” Ted Kennedy, health care reform became a dying cause, and in his posthumous note to President Obama, he poignantly wrote: “What we face is above all a moral issue; at stake are not just the details of policy, but fundamental principles of social justice and the character of our country…health care reform…is the great unfinished business of our society.”
Canadians who watch the latest chapter in the American experiment and cluck about its excesses would do well to remember that the founding fathers desired a system constructed on checks and balances and conditioned by open and lively argument. The American political system is more sophisticated (often to its detriment) than the Canadian one and the number of interests that must be reconciled several orders of magnitude greater than in the Canadian one. The health care debate illustrates all these features. It is also a revelatory look at the polarization between the parties and the factionalism within the parties, and into the Washington world of lobbyists and lawyers, interest groups and advocacy. The debate in the US provides an instructive insight into the American process that Canadians should watch and profitably learn from, because if you want to play in the American system, you need to learn to play by American rules.
Canadians should also pay attention because the American experiment is one of constant innovation and invention. Health care, thanks to biotechnology and life-changing projects like the human genome, is going through a remarkable revolution that will literally change how we live and how long we live. The practical application, already begun, of some of the Obama-inspired innovations — billions for the development of an e-health infrastructure (Ontario, take note), as well as the massive continuing investments into research, are already affecting our increasingly integrated pharmaceutical and medical research industries as well as health care delivery. For example, the development of standards for the secure exchange of health information will likely become the norm throughout Canada and the US.
Politically it is extraordinarily ambitious. It means taking on a sector that represents one sixth of American GDP and interests that include the medical profession, drug industry, insurers and seniors. Reform would change the lives of all Americans, especially the more than 133 million Americans living with chronic diseases and disabilities and their family caregivers.
America’s is the most expensive system in the world. Health insurance premiums in states have gone up between 90 and 150 percent over the last decade — far faster than wages and inflation. It is currently devouring between 18 and 19 percent of their GDP, yet it leaves as many as an estimated 50 million Americans without insurance.
Obama campaigned on a platform of expanding health care and improving the delivery system. He wants to change the US system and the way the money flows through it. He’d put the emphasis on prevention and maintenance rather than costly repair in hospitals. Initially agnostic about public insurance plans to compete with the current system of private plans, in deference to the pressure of liberals and labour, who have long campaigned for universal coverage and a public option, Obama has embraced the “public option” — a government-administered health plan that the insurance companies argue will constitute unfair competition. In an effort to placate the insurers, he has argued that the new scheme must be mandatory and require the young and healthy to pay premiums to balance out the costs of coverage for the sick and elderly.
The most important lesson of the Clintons’ 1993-94 failed effort, labelled “Hillarycare,” was the requirement to respect the authority of the legislative branch. Having sketched out his requirements Obama left it to congressional leadership, most of them oldline liberals, to put together the reform bill.
The bills emerging from congressional committees in the House and Senate would extend coverage to all Americans. They would include a tax on the wealthy, tax credits for low- and moderate-income individuals, penalties for people who do not purchase coverage and a public insurance option, perhaps regional coops, pegged to Medicare reimbursement rates, and triggered if the private insurance system does not work. They would oblige employers to provide insurance and require those without coverage to acquire it. Medicaid would cover the poor and insurance companies would not be able to reject anyone, regardless of pre-existing conditions.
Critical to congressional resolution is the fate of the “public option.” The challenge for Obama is to find a compromise between liberals who demand a public option and cost-conscious centrists who call it a deal-breaker. It is integral to the various House and Senate bills, with the exception of that of the Senate Finance Committee. Its chair, Montana Democrat Max Baucus, best known to Canadians for his aggravating behaviour on softwood lumber, is convinced a public option does not have sufficient legislative support. Importantly, the Baucus Bill is the only one that the Congressional Budget Office estimates would be deficit-neutral, because it includes realistic taxing provisions.
Assuming a reconciliation of the various bills — three from the House and two from the Senate, in a joint House-Senate conference and then passage by both chambers (including a 60-vote majority to make it filibuster-proof in the hundred-seat Senate) — the Bill could still meet the presidential wish for a signature before Christmas. Then will come the truly heavy lifting, keeping mind of the problems encountered when rolling out the extension of pharmacare in the Bush administration.
Although most of the bill’s provisions won’t likely take effect for three or four years, the various agencies and departments of the administration must begin its implementation, including funding authorizations, in coordination with the insurance companies and health care operators, as well as state and local governments.
The debate, as David Blumethal and James Morone point out in The Heart of Power: Health and Power in the White House, reflects the classical divide in the American polity between liberals, who imagine a universal right to health care tied to compulsory insurance, like that of Social Security, and conservatives, who are satisfied with the current model of a market-based system for health care based on private insurers and employers with the right to opt out.
The health care fight is also a clash over money — or, more to the point, who pays for it? The Department of Health and Human Services reckons health care will cost each American over $8,000 this year (for Canadians it is about $5,000). The Congressional Budget Office’s original estimates of the Obama reforms put the cost at a trillion dollars over the next decade. Half the revenue would come from a tax increase on the wealthiest 1 percent of Americans and corporations, and the remainder from cost-savings to a reformed Medicaid and Medicare.
The recession may be decelerating, but the economy is still trending downward, threatening Obama’s approval rating. Popular anxiety about deficits and debt is also rising. The linkage between health care and the deficit is central to the morality stakes over entitlement versus affordability. Bank bailouts, stimulus spending and declining tax revenues due to a deep recession led the government to post a deficit of $1.4 trillion — 9.9 percent of the US GDP for the 2009 fiscal year that ended September 30. The deficit for fiscal 2008 was $459 billion.
There continues to be broad public support for the idea of reform, but the Obama administration has not yet connected its plan to increased security for the middle class, nor has it persuaded the insured that their current benefits will not be adversely affected. Medicare beneficiaries are worried their health care program will be cut to subsidize coverage for the uninsured.
Public opinion on health care is complex. It varies and conflicts depending on age, income and geography, with divisions on what priority to emphasize, how fast to act and what is important to protect. Surveys show, for example, that seniors are the most anxious over health care reform. They vote in larger numbers than any other demographic.
Historically, conservatives object to social security and Medicare, arguing that government takeover will limit Americans’ ability to choose their doctors and course of treatment; then there is the cost factor. The Republicans have opposed almost everything that Obama and the Democratic leadership have proposed. Their alignment with the relentless attacks of those interests opposed to the reform, whether because of specific provisions or in principle, has had an effect.
Public opinion surveys increasingly indicate that “Obamacare” threatens to hang like a noose around the neck of the Democrats.
The Republicans remember how defeating Bill Clinton’s health care reform set the stage for taking over Congress in 1994. They are gambling that history will repeat itself in the 2010 midterms.

The inner workings of government
Who’s doing what to get federal policy made. In The Functionary.
The inner workings of government
Who’s doing what to get federal policy made. In The Functionary.
Concerned that their party may prevent progress on one of the nation’s most intractable problems, state governors like California’s Arnold Schwarzenegger and former Washington power-brokers, including two former Senate majority leaders — Bill Frist and Bob Dole (who was the GOP presidential candidate in 1996) — and former health and human services secretary Tommy Thompson, are calling on their fellow Republicans in Congress to help pass a health care bill. But they are the exception, and in committee stage, only one lone Republican, Senator Olympia Snowe of Maine, heeding “history’s call,” supported the Baucus Bill.
Republican opposition is a reflection of the polarization that now characterizes American politics, notwithstanding the promise of Inauguration Day for a renewal of bipartisanship. Instead, as Washington Post columnist E. J. Dionne observes:
Democrats see Republicans as a collection of pampered rich people who selfishly seek to cut their own taxes, joined in alliance with religious fundamentalists who want to use government power to impose a narrow brand of Christianity on everyone else. Republicans see Democrats as Godless, overeducated elitists who sip lattes as they look down their noses at the moral values of “real Americans” in “the heartland” and ally themselves with “special interest groups” who benefit from “big government”…The divide in American politics is about more than the ideological distance between the two parties. Right now red-staters and blue-staters live in two different political universes. It’s no wonder that political moderation is out of fashion.
With the Republicans refusing their support, the congressional battle is now within the Democratic caucus and over who and how Americans will foot the bill.
Unlike the Canadian system, party loyalty in the US is more of a label than a brand. Legislative success depends on the construction of coalitions that are built around region, industry and local interests, and each chamber has its own dynamic. Political scientist Nelson Polsby likened the Senate to a “carpool,” solicitous of individual members, while he described the House as more like a “bus line,” scheduled and controlled by its leadership.
Understanding the congressional system is critical to Canadian advocacy efforts — shifting coalitions and the differences in each chamber means that we have to work members of both parties based on their interests. We also need to remember that there are no permanent friends or enemies. As I noted in the early 1980s, Senator Moynihan was our ally on acid rain but an adversary on Buy America — a reminder that all politics are local.
Within each party are caucuses united by ideology, ethnicity or geography, and Canadians also need to better understand these beasties if we are to effectively position our own interests. The 81 House members affiliated with the Progressive Caucus of the Democratic party have worked throughout its history for enactment of a single-payer, Canadian-style health care legislation, in tandem with the 68 members of the New Democratic Coalition.
But the critical bloc in the health care debate is the 52 member Blue Dogs, Democrats from small towns and rural America in the midwest and south, who draw their unity from their fiscal conservatism and their concern that their party leadership, drawn from the big cities on the west coast and northeast, is both too liberal and too attached to big government.
Reflecting their swing status, the Blue Dogs have set a record pace for fundraising this year, raising more than half their money from the health care, insurance and financial services industries. Their fundraising effort provides a further insight into the American process and the money imperative of politics, which effectively requires each member of Congress to raise $5,000 every working day to be sufficiently financed for their biennial campaigns. Senate races, held every six years, cost much more — averaging around $15 million (or about what the Liberal Party of Canada spent in 2008 on its entire campaign). As acting chairman of the Senate Health, Education, Labor and Pensions (HELP) Committee, filling in for the ailing Ted Kennedy, Connecticut Democrat Chris Dodd tapped health-care-related companies for more than $112,000 during the second quarter of 2009.
Understanding the congressional system is critical to Canadian advocacy efforts — shifting coalitions and the differences in each chamber means that we have to work members of both parties based on their interests. We also need to remember that there are no permanent friends or enemies.
Obama’s promise to “clean up” Washington and “eliminate special interests” notwithstanding, money and interests keep the Capitol’s merry-go-round turning in the belief that one person’s special interest is another’s job or moral crusade. Lobbying is as old as the Republic. In 2008, according to the Center for Responsive Politics, there were over 16,000 active registered lobbyists — persons with sufficient congressional contacts that by law they’re required to report. This number represents an increase of about 50 percent since 1998. It does not include the legions of public relations consultants, advertising managers, Internet advisers and policy experts, who are primed to influence government. Include these in the mix, and political scientist James Thurber of American University reckons the influence-lobbying complex in Washington is closer to a quarter million people. Under activist government, these numbers are expanding.
In the months after the November election and in anticipation of the stimulus package, more than 2,000 cities and states, companies and associations hired lobbyists to help them push their agendas on Capitol Hill and at the
White House. The capital’s politics, as well as its restaurants, thrive on lobbying, armored comfortably, if not always virtuously, by the constitutional Second Amendment’s guarantee of freedom of speech. Leading lobbyist Heather Podesta, the sister-in-law of Obama transition director and former Clinton chief-of-staff, John Podesta, once issued an invitation to a fund-raiser promising a lunch that was supposed to consist of “the Select Committee on Intelligence for the first course followed by your choice of Appropriations, Judiciary or Rules committees.” The Washington Post sniffed that the invitation was in “poor taste,” but that is the way Washington works.
For K Street, the bustling intersection of money and politics from where most lobbyist and lawyers sally forth, health care has become this year’s principal cause and its main source of enrichment. And it gets the job done. Lobbying on behalf of medical research institutions, for example, helped to persuade Congress to include an additional $10.4 billion for the National Institutes of Health (NIH) in the stimulus bill. Earmarks, what the late William Safire described in his Political Dictionary as “funds that individual senators or representatives specify be directed to projects and activities that will benefit particular people, institutions or locations in their home constituencies” have ballooned. In 2008, the Center for Responsive Politics estimated, spending bills included $18.3 billion in earmarks; for 2009 the count in the “Congressional Pig Book” has already topped $20 billion.
With the health care campaign already saturating the national airwaves, it has the potential to become the mother of all advocacy ad wars. The drug industry, already the biggest-spending lobby in Washington, spent $47.4 million on lobbying in the first three months of 2009. Much of the money is spent on advertising through the media. According to the Campaign Media Analysis Group, during the first half of 2009, $31 million was spent for roughly 47,000 TV ads on health care. That’s double the roughly $14 million the insurance industry spent in 1993 and 1994 for the famous “Harry and Louise” ads, which are credited with helping kill President Bill Clinton’s health care drive, but a fraction of the $250 million the group reckons will ultimately be spent in 2009. Political advocacy ad buys this year are expected to exceed $1 billion.
It is in the advertising war that Canada enters the fray, with Shona Holmes, the Ontario woman who sought treatment in the US, having replaced “Harry and Louise” (who have returned this year in an ad arguing for reform) as the poster child for the antireform movement, which decries Canada’s lack of choice, totalitarian administration, and “millions” awaiting treatment. Then there is our “parasitic” prescription drug culture, which depends on the US to do “all the innovation,” as Tennessee Republican senator Bob Corker pronounced at a September congressional hearing.
The American pharmaceutical industry has long lobbied against the import of cheaper generics from Canada. When I was in Los Angeles as our consul-general and did talk radio, I could always count on at least one apocryphal story about a mythical person who had died from “cheap Canadian drugs.” The questioning was predictable: “What about those ”˜bad’ generic drugs that you have to use?” So was my response predictable: “We use the same generic drugs, usually imported from Ireland or India, and we buy in bulk, like the Veterans Administration and did you know that the infant mortality rate in the US is 40 percent higher than Canada’s, and American mothers are 57 percent more likely to die in childbirth? And our seniors live longer.” As an antidote to the mythology and urban myths being propagated in the US, the Canadian Medical Association could do some useful education about our system.
If political afterlife in the Canadian system is a government appointment, in Washington the path from defeat or retirement leads in most cases to K Street. About one-quarter of the House and Senate members who retired or lost elections last year have found new jobs with lobbying firms. Bloomberg reports that of the 2,737 lobbyists hired to promote the interests of drug companies, insurers, hospitals, health professionals, industry groups and business organizations, 1,418 — or 52 percent — have worked for Congress, the White House or federal agencies. Among the 55 former members of Congress is Billy Tauzin, who represented Louisiana in the House for more than two decades, first as a Democrat and then as a Republican, and who now heads PhRMA, the leading drug lobby. With the Democratic ascendence in Congress and in the Obama administration, the going rate for former Democratic staffers is $500,000 a year and up more former top aides, and more junior staffers are fielding offers ranging from $120,000 to $200,000.
While Congress is the main theatre of action, the battle for public opinion stretches beyond the Beltway and Obama is actively using the bully pulpit of the presidency to convince skeptical Americans that a new system would actually help them, not limit their choices and care.
The second lesson of the 1993-94 health care debacle was: Know your audience — insured taxpayers. Former majority leader Tom Daschle, Obama’s first nominee for health and human services secretary, until controversy over forgetting to pay taxes on his limousine and driver obliged him to withdraw, has written a useful primer for this season — Critical: What We Can Do About the Health-Care Crisis (2008). In it Daschle argues that the Clintons’ approach to reform failed to appreciate that “many people who have insurance now are satisfied with it, and are wary of changes.”
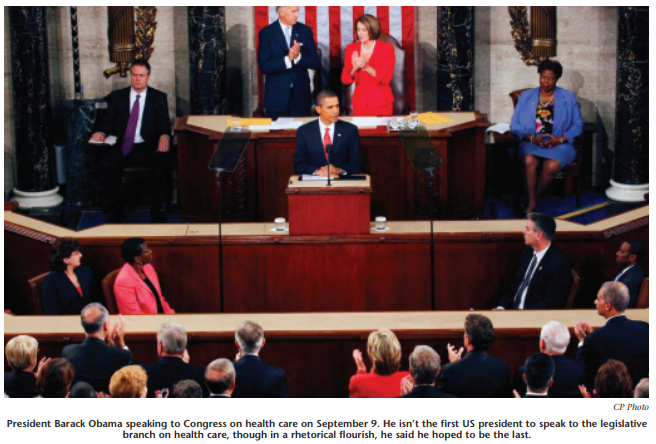
While Congress is the main theatre of action, the battle for public opinion stretches beyond the Beltway, and Obama is actively using the bully pulpit of the presidency to convince skeptical Americans that a new system would actually help them, not limit their choices and care. In his September 9 speech, his first to a joint session of Congress, he answered critics who say his plan was too expensive by pointing out that his $900 billion health care plan would actually cost less than America has spent on two wars and on Bush administration tax cuts. Obama followed it up with an unprecedented appearance on all five Sunday morning talk shows. In early October he appeared in the Rose Garden with 150 white-coated physicians in a direct effort to associate his health care plan with the most publicly trusted figures in the debate.
Technology, coupled with the Obama appeal, created for him a political organization like no other — barackobama.org is a Facebook page of 13 million activists, which Obama he has entrusted to his principal campaign organizer, David Axelrod. It was critical to Obama’s election but despite its employment on the stimulus package and health care its utility as a legislative enabler is unproven. Governing lacks the romance of the first-time election campaign and legislating, as has been often observed, is like making sausage.
Before the August break, the chief aides to Senate Democrats met in a nondescript Senate conference room with three former advisers to President Bill Clinton to go over the lessons of the 1993-94 failure. In addition to leaving the details to Congress and making insured taxpayers a prime target, they concluded that delay only whittles away your support, so that sooner than later “you need to take what you can get.”
To recapture the initiative, the White House is arguing that reform will be fully funded, will not jeopardize current doctor-patient relationships, and is the only alternative to the current, broken system. But the trillion-dollar question remains: without adding to already huge deficits, can President Obama find that much in spending cuts and tax increases to overhaul the health care system?
The Obama team can take encouragement from the Canadian experience with change and reform. The debate during the 1960s over the Pearson-era reforms, which changed our flag, our labour code and our pension scheme and enacted Medicare, was fierce and heated, but as Tom Kent would later observe in his memoir A Public Purpose (1988), the reforms soon “fitted into the fabric of Canadian society as if it had always been there.” Kent concluded: “it is hard to think of anything of comparable significance to people about which there has been so little subsequent controversy.”
Photo: Shutterstock

